Lower the risk of getting malaria by avoiding mosquito bites: Use mosquito nets when sleeping in places where malaria is present. Use mosquito repellents (containing DEET, IR3535 or Icaridin) after dusk. Use coils and vaporizers. Wear protective clothing.
Setting goals and striving to meet them can be good for kids. But extreme content on social media can push them toward unrealistic standards that encourage dangerous habits. A few examples of social media-fueled trends that may have unhealthy effect on body image:
Bigorexia, a condition that drives young people to spend countless hours in the gym and eat a protein-heavy diet to build a “jacked” body.
Diphtheria is a serious, potentially life-threatening bacterial infection that primarily affects the nose and throat, but can also affect the skin. It is caused by the bacterium Corynebacterium diphtheriae, which produces a toxin that damages the respiratory tract and can spread to other parts of the body.
Autism spectrum disorder (ASD) is a neurodevelopmental condition defined by impairments in social communication and the presence of restricted interests and repetitive, stereotyped behaviors or activities.
Autism spectrum disorder (ASD) represents a substantial public health concern with global relevance, affecting individuals across diverse ethnic, geographic, and socioeconomic backgrounds. Despite its widespread prevalence, effective treatment options remain costly, and no definitive cure has been identified. Moreover, the level of awareness and understanding of autism continues to be limited and highly variable, often influenced by factors such as educational attainment and national context.
Autism spectrum disorders (ASD) encompass a range of conditions linked to brain development that impact an individual’s social interaction, communication abilities, along with distinctive behavioral and activity patterns. These may involve challenges with transitioning between tasks, an intense focus on details, and atypical sensory responses (World Health Organization, 2022). Autism spectrum disorders (ASD) have a strong genetic basis with over 100 genetic polymorphisms linked to the condition. Notably, Africa possesses greater genetic diversity than any other continent. However, environmental risk factors for autism remain poorly understood (Eze, 2018).
Autism Spectrum Disorder (ASD) is recognized as a global health concern, with an estimated 52 million individuals affected worldwide. Current global prevalence is reported at approximately 0.6% (95% CI: 0.4–1%), with children constituting about 1–2% of this population. Notably, the condition affects approximately 1 in 160 children globally, with boys being disproportionately more affected than girls. These statistics highlight the widespread nature of ASD and its growing significance in child health worldwide (Ayobami Adesoji Aiyeolemi et al., 2024; Salari et al., 2022; Reddy, Fewster & Gurayah, 2019). Parents usually notice signs in the first two or three years of a child’s life. These signs often develop gradually, though some children with autism reach their developmental milestones at a normal pace and then worsen (Eze, 2018).
In contrast, early studies once suggested that autism might be a culturally bound or even rare disorder in regions such as Africa. However, this assumption has been increasingly challenged by growing documentation of ASD cases across various African countries, including Kenya, Zimbabwe, Nigeria, and Ghana (Eze, 2018). These reports highlight that autism is not rare but rather under-recognized, often due to limited diagnostic capacity, low awareness among caregivers and professionals, and prevailing cultural beliefs. Despite the presence of ASD, systemic and social barriers continue to hinder early detection and access to appropriate services.
While global research on ASD has expanded, significant knowledge gaps persist—particularly in low- and middle-income countries. In the African context, there is a lack of reliable data on ASD prevalence, limited understanding of public and professional awareness, and scarce evaluation of intervention models suited to local needs. Misconceptions and stigma further contribute to delayed diagnoses and inadequate support systems.
Autism Spectrum Disorders (ASDs) are of significant global public health importance, as their symptoms often lead to considerable impairments in a child’s overall functioning. To address these challenges, raising awareness, early recognition, and timely intervention are highly recommended. However, in resource-limited settings, many individuals with ASD go undiagnosed, misdiagnosed, or are diagnosed late, often lacking access to essential services due to limited awareness, particularly among parents, health professionals, and teachers. This lack of understanding fosters negative attitudes toward people with ASD, while the absence of appropriate interventions worsens the situation.
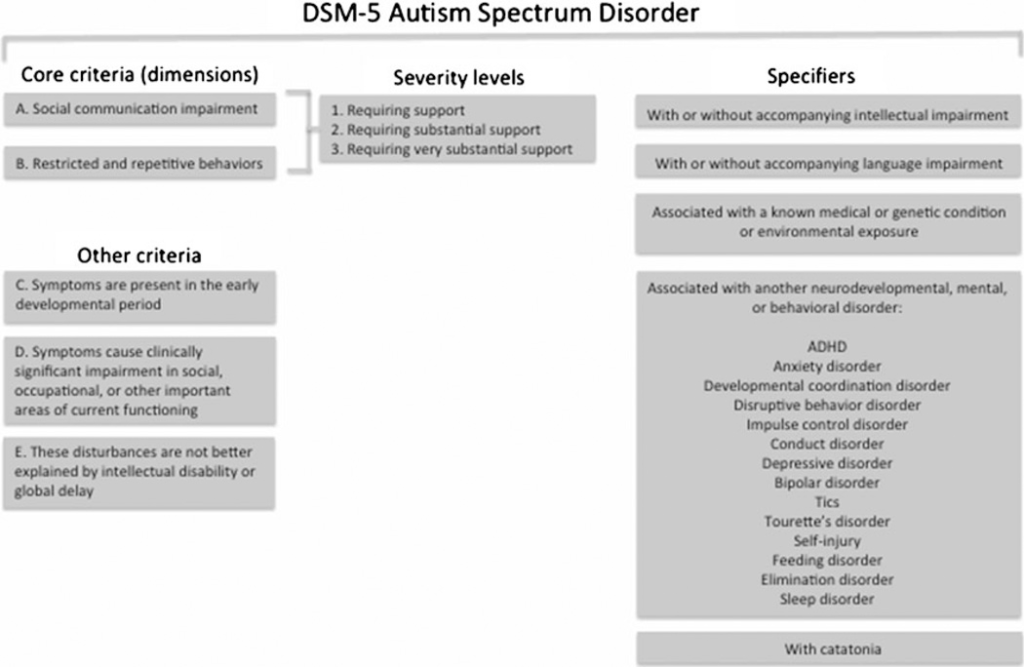
CLASSIFICATION OF AUTISM SPECTRUM DISORDER
The DSM-5 diagnostic criteria for ASD include:
Persistent deficits in social communication and interaction across various contexts.
Restricted and repetitive patterns of behavior, interests, or activities, either currently observed or reported in clinical history.
Clinically significant impairment in social, occupational, or other essential areas of functioning.
Symptoms present from early childhood, though they may not become fully evident until social demands exceed the child’s abilities.
Symptoms not better explained by intellectual disability or global developmental delay.
(Ousley and Cermak, 2013)
RISK FACTORS
a. Genetic Factors
Heritability estimates for autism spectrum disorder (ASD) vary widely, ranging from 37% to over 90%, based on twin studies. A more recent five-country cohort study estimated the heritability of ASD at approximately 80% (American Psychiatric Association, 2013).
Concordance rates for ASD are significantly higher in monozygotic (identical) twins, ranging from 36% to 96%, compared to 0% to 27% in dizygotic (fraternal) twins. Additionally, the likelihood of autism is 50 to 200 times greater in siblings of autistic individuals than in the general population. Even among relatives of individuals with ASD who do not have the condition themselves, there is a higher prevalence of milder communication and social skill difficulties.
Ongoing research is investigating the genetic mechanisms underlying ASD through whole genome screening, cytogenetic analysis, and candidate gene studies. Findings suggest an increased risk of ASD associated with gene variants on chromosomes 2, 3, 4, 6, 7, 10, 15, 17, and 22. Cytogenetic studies have also identified abnormalities at the 15q11-q13 locus in individuals with ASD.
Genome-wide association studies (GWAS) have identified genetic variants at the 5p14.1 and 5p15 loci as having slight effects on ASD risk. Additionally, specific copy number variations (CNVs), which occur more frequently in individuals with ASD than in control groups, have been detected at chromosome regions 1q21, 2p16.3, 3p25-26, 7q36.2, 15q11-13, 16p11.2, and 22q11.2 (Fuentes et al., 2014).
b. Neuroanatomic and Neuroimaging Findings
While not diagnostic, neuroanatomic and neuroimaging studies have consistently shown increased cerebral volume in individuals with autism spectrum disorder (ASD), affecting both grey and white matter, along with enlarged ventricles. Additional neuroimaging findings include abnormalities in brain chemistry, serotonin synthesis, and brain electrophysiology.
Postmortem studies of young children with ASD have identified discrete patches of disorganized cortex in the majority of samples. These abnormalities are primarily located in brain regions responsible for social interaction, emotional regulation, communication, and language—functions that are typically impaired in autism. Such findings suggest a common set of developmental neuropathological features associated with ASD, likely resulting from disruptions in cortical layer formation and neuronal differentiation during prenatal development (Fuentes et al., 2014).
Several environmental factors have been linked to a higher risk of developing autism spectrum disorder (ASD). These include maternal exposure during pregnancy to harmful substances such as heavy metals (e.g., mercury, cadmium, nickel), industrial chemicals (trichloroethylene and vinyl chloride), infections such as rubella and influenza. Nutritional deficiencies, particularly in folic acid, may also contribute to increased risk. Other contributing factors include advanced parental age, extreme prematurity, and prenatal exposure to certain medications or teratogens, including valproic acid and opioids. These factors are believed to impact fetal brain development and the nervous system’s maturation, potentially increasing susceptibility to ASD (American Psychiatric Association, 2013; Qin et al., 2024).
Beyond genetic and environmental influences, epigenetic mechanisms also appear to play a role in ASD. Several genetic syndromes that frequently co-occur with ASD exhibit dysregulation of epigenetic markers, which are critical in regulating gene expression. Research into epigenetics offers a potential framework for understanding the reported increase in autism prevalence suggested by epidemiological studies (Fuentes et al., 2014).
e. The NICE (2011) guideline on Autism: Recognition, Referral, and Diagnosis of Children and Young People on the Autism Spectrum highlights several clinically and statistically significant risk factors for autism spectrum disorders (ASD), despite the overall low quality of evidence. These risk factors include:
Having a sibling with autism or another ASD
Parental history of schizophrenia-like psychosis, affective disorders, or other mental/behavioral disorders
Maternal age over 40 years
Paternal age between 40–49 years (ASD) or over 40 years (autism)
History of threatened abortion before 20 weeks gestation
Residence in a capital city or its suburbs
Medical Conditions Associated with ASD
The NICE guideline also lists several medical conditions with a noted prevalence of ASD, again with the caveat of low-quality evidence:
Intellectual disability (8%–27.9%)
Fragile X syndrome (24%–60%)
Tuberous sclerosis (36%–79%)
Neonatal/epileptic encephalopathy or infantile spasms (4%–14%)
Cerebral palsy (15%)
Down syndrome (6%–15%)
Muscular dystrophy (3%–37%)
Neurofibromatosis (4%–8%)
DIAGNOSTIC TOOLS FOR AUTISM SPECTRUM DISORDER (ASD)
Diagnostic tools for ASD range from traditional behavioral assessments to emerging technologies. These tools differ in accuracy, accessibility, and suitability across contexts.
Traditional Diagnostic Methods Conventional approaches rely on detailed behavioral evaluations and developmental histories, typically conducted by pediatricians, psychiatrists, or neuropsychologists. These include direct observations and interviews with caregivers to assess a child’s communication, social interaction, and behavioral patterns (Tanu & Kakkar, 2019).
Countries like Spain and Ireland have adopted early screening tools such as the Modified Checklist for Autism in Toddlers (M-CHAT), targeting children aged 18–30 months. However, these tools may lack sensitivity and often depend on parental concerns before ASD is suspected (Lordan et al., 2021).
Differential Diagnosis of Autism Spectrum Disorder (ASD) according to DSM 5
Neurodevelopmental Disorders
ADHD: Both ASD and ADHD may involve attention abnormalities and social communication difficulties. However, ASD includes restricted, repetitive behaviors, which are absent in ADHD. A dual diagnosis may be appropriate if attentional issues or hyperactivity exceed typical levels
Intellectual Developmental Disorder (IDD): Differentiating ASD from IDD can be challenging, especially in young children. A diagnosis of ASD is appropriate when social communication is significantly impaired relative to the individual’s nonverbal skills.
Language Disorders & Social (Pragmatic) Communication Disorder (SPCD): While language disorders may cause communication difficulties, they lack the repetitive behaviors seen in ASD. If restricted/repetitive behaviors are present, ASD takes precedence over SPCD.
Selective Mutism: In selective mutism, children communicate appropriately in some settings but remain mute in others, without the social impairments and repetitive behaviors seen in ASD.
Movement and Genetic Disorders
Stereotypic Movement Disorder: Motor stereotypies occur in both disorders. However, if repetitive behaviors are better explained by ASD, an additional diagnosis of stereotypic movement disorder is unnecessary unless self-injury is significant.
Rett Syndrome: Social withdrawal is seen in the regressive phase of Rett syndrome (ages 1–4). However, most individuals later regain social communication skills, unlike ASD.
Psychiatric Disorders
Anxiety Disorders: Social withdrawal and repetitive behaviors in ASD may overlap with anxiety disorders. Specific phobias, social anxiety, and agoraphobia are commonly comorbid with ASD.
Obsessive-Compulsive Disorder (OCD): Both OCD and ASD involve repetitive behaviors, but in OCD, these are driven by intrusive thoughts and anxiety relief, whereas in ASD, they are often pleasurable and routine-based.
Schizophrenia: Childhood-onset schizophrenia follows a period of typical development and features hallucinations and delusions, which are absent in ASD. However, individuals with ASD may misinterpret questions about psychotic symptoms (e.g., mistaking radio voices for hallucinations).
Personality Disorders: Traits of narcissistic, schizotypal, or schizoid personality disorders may resemble ASD in adults. However, ASD is characterized by early childhood impairments in imaginative play, sensory sensitivities, and repetitive behaviors, which differentiate it from personality disorders.
Proper differentiation ensures accurate diagnosis and appropriate intervention for individuals presenting with ASD-like symptoms.
TREATMENT OF AUTISM SPECTRUM DISORDER (ASD)
Treating ASD is a multifaceted process that must be tailored to each individual’s unique needs. Factors such as age, symptom severity, co-occurring conditions, family dynamics, availability of services, and cultural background all play a role in shaping an effective treatment plan. While there is no universal “cure” for ASD, the aim of treatment is to be personalized, context-sensitive, and empowering, helping each person reach their fullest potential.
a. Applied behavior analysis (ABA) ABA is a structured, evidence-based therapy that focuses on enhancing a child’s specific abilities by addressing key areas such as social interaction, communication, academic performance, and daily living skills, while also working to reduce harmful or disruptive behaviors
b. Social Skills Training (SST) Social skills training is designed to help children with Autism Spectrum Disorder (ASD) enhance their ability to engage in everyday social interactions. It focuses on building essential skills such as understanding social cues, effective communication, and forming meaningful relationships (Liu, 2023).
2. Medical Treatment: Medication for Autism Spectrum Disorder (ASD)
While there is no medication that cures ASD, certain drugs can help manage specific co-morbid conditions such as behavioral challenges, attention difficulties, anxiety, and mood instability. Medication is typically part of a broader, individualized treatment plan aimed at enhancing overall functioning and quality of life.
3. Biofeedback and neuromodulation in ASD Treatment
Biofeedback and neuromodulation are an emerging, non-invasive therapeutic strategies aimed at enhancing brain function and alleviating symptoms in individuals with Autism Spectrum Disorder (ASD). These approaches focus on helping individuals gain better control over physiological processes and brain activity.
4.Diet and Nutrition Interventions Diet and nutrition are gaining attention as supportive strategies in ASD management. Some children with ASD may experience symptom relief from specific dietary changes, such as gluten-free, casein-free (GFCF) diets, which may help reduce behavioral and gastrointestinal issues.
Nutrient supplementation—particularly omega-3 fatty acids, zinc, magnesium, and certain vitamins—has also shown potential in supporting brain function and reducing ASD symptoms. However, responses vary widely, and the evidence remains inconclusive.
5 Social and Educational Integration
a. Educational Integration of Children with ASD Inclusive education integrates children with ASD into mainstream classrooms, promoting academic progress and social development alongside their peers. Individualized education plans, adaptive teaching methods, and in-class support—such as speech therapy or behavioral interventions—help meet each child’s unique needs.
b. Social Integration and Employment of Adults with ASD Many adults with ASD face challenges in social participation and securing employment. Yet, there is growing recognition of their strengths and contributions in the workplace. Inclusive practices such as flexible roles, clear communication structures, and on-the-job support are improving opportunities.
c. Community-Based Support: Local support services and coordinated efforts among various agencies can play a vital role in helping individuals with ASD achieve their full potential.
d. Family Involvement: Families are essential to the success of interventions and should be equipped with proper training, access to respite care, and ongoing social support services.